This is the ultimate guide and review of Cardarine, also known as GW 50156 or Endurobol. A compound that is commonly mistaken to be a SARM but it’s actually not.
In this guide / review, you will learn:
- What is Cardarine and how does it work
- Benefits, side effects
- Is Cardarine legal
- Can Cardarine cause cancer
- Lots, lots more
Keep in mind that Cardarine is considered to be a research compound and is not approved for human consumption. Don’t take the information you find here as medical advice, you should always talk to your doctor.
My recommended companies for buying Cardarine
If you are in a rush and don’t have time to go over this article, check out this video. It’s not as in-depth but it goes over the important things about Cardarine.
https://www.youtube.com/watch?v=doCDG-FNE2s&feature=emb_title
Let’s start off by explaining what Cardarine actually is and how it works.
What is cardarine (GW 50156)
Cardarine is frequently mistaken to be a SARM (Selective Androgen Receptor Modulator). This is absolutely not the case.
In reality, GW 50156 is actually a PPARδ receptor agonist (Peroxisome proliferator-activated receptor delta agonist) and not a SARM at all.
It provides benefits like:
- Increased endurance
- Improved cardiovascular health
- Fat loss
We will go over all the benefits of Cardarine in more detail later in the article.
Cardarine history
GW 50156 was designed in the 90s by Ligand Pharmaceuticals and GlaxoSmithKline to treat diseases like diabetes and cardiovascular diseases. If the name Ligand Pharmaceuticals sounds familiar to you, that’s because they developed and named LGD 4033.

Cardarine went through a lot of studies and trials but the compound was ultimately abandoned in 2007 when a study was done by GlaxoSmithKline that showed cancer development in rats. More on this later.
After that, a lot of people discussed this and even some studies were done that have contradictive results (we will talk more about that later in the article).
Even though Cardarine got abandoned because of safety concerns, athletes, bodybuilders, and others started using it because of the amazing endurance benefits and fat loss it provides. Some people also use it to improve their cardiovascular health.
Shortly after people started using this compound, the WADA ( World Anti Doping Agency) added Cardarine and other PPARδ receptor agonists to the banned substances list.
How does Cardarine work
As we said, Cardarine is a PPARδ receptor agonist. This means that it binds to the PPARδ receptor to trigger some biological responses.
The main results of Cardarine binding to the PPARδ receptor are:
- Increased oxidative capacity in muscles (This means more fat loss and a great increase in endurance)
- Switching our energy source from glucose to fat (suppression of Glucose metabolism)
Scientists and athletes are most interested in the Glucose metabolism suppression effect that Cardarine has. Athletes love this because it’s one of the main reasons for the incredible endurance increase benefit that Cardarine provides.

Scientists on the other hand, are very interested in this because it results in an increase in insulin sensitivy. This means that Cardarine has the potential to treat Diabetes.
Glucose metabolism suppression essentially means that the body starts using fat as an energy source instead of fat. Because of this, a lot of people started using Cardarine to help them lose body fat easier.
We will go over each benefit as well as the side effects and explain them in detail later in the article.
Cardarine legal status
Let’s clear this up right away, as of April 2024, Cardarine is legal to buy and use in every country in the world except for Australia. We will go over the legality in Australia later in the article. It’s also a little different in professional sports, we will go over that as well.
GW 50156 is sold under the labels of “Research Chemical” or “Not for human consumption” because it’s not FDA (Food and Drug Administration) approved for human consumption. This, however, doesn’t have anything to do with Cardarine being legal or illegal.
To summarize, Cardarine (GW 50156) is legal to buy and use in every country in the world with the exception of Australia. Now, let’s go over the legality of Cardarine in Australia.
Cardarine in Australia
As we said, when it comes to the legality of Cardarine, Australia’s laws are a little different from the rest of the world.
In Australia, Cardarine is considered to be a Schedule 9 compound by the TGA. This means that it’s illegal in Australia even with a doctor’s prescription. Fun fact, Cocaine is also considered a Schedule 9 drug in Australia.
SARMs and MK 677, however are legal in Australia with a doctor’s prescription.
Even though Cardarine isn’t legal in Australia, a lot of Australians frequently use it.
You can read more about this in my article on SARMs in Australia.
Cardarine in sports
Cardarine (GW 50156) is considered a prohibited substance for professional athletes by almost all sports bodies, including the Olympics because of the obvious unfair advantages that it gives (endurance increase).

GW 50156 is on the list of banned compounds by the USADA (the United States Anti Doping Agency) as well as the WADA (World Anti Doping Agency) and the ASADA (the Australian Anti-Doping Agency).
If you want to read more about this subject, read our article where we answer the question; is Cardarine legal.
Cardarine benefits
As we said, GW 50156 has great benefits of fat loss, increased energy, an incredible increase in endurance, improved cardiovascular health and more.
Full list of Cardarine benefits:
- increased endurance
- fat loss
- improved cardiovascular health
- improved kidney and liver health
Now let’s go over each benefit in more detail.
Increased endurance
As we said earlier in the article, Cardarine actually increases our endurance in two different ways:
- Suppression of Glucose metabolism (switching energy source from glucose to fat).
- Increased oxidative capacity in muscles.
Both of these together result in a serious increase in endurance. Most people are able to increase their endurance by up to 60% after about 30 minutes from their first Cardarine dosage. Insane, right?
Rat studies actually proved this benefit. The studies showed that the group of rats that were taking Cardarine almost instantly had 50-70% more endurance than the other rats. In other words, it took them almost twice as long to get tired.

Unsuprisingly, a lot of athletes take GW 50156 just because of this benefit. Sadly, a lot of professional athletes use it as well to get an edge over their competition. In fact, Lance Armstrong is said to have used Cardarine as well as Stenabolic (a similar compound that increases endurance) to be able to win Tour de France 7 times.
You can expect to see increased endurance 30 minutes after your first dosage. You will get even better endurance week after week if you run and train hard. And the best thing about this is, you can keep most of the endurance you gained during your Cardarine cycle if you continue to train and run after the cycle is over.
Most people instantly see around a 50 – 60% endurance increase. This means that if you are able to run 2 miles, you will easily be able to run 3 miles after the first dosage. A lot of people even say that being on GW 50156 feels like you have three lungs because you can breathe so easily.
You won’t notice it only when running, you will also see the increased endurance when lifting weights. You won’t need as much rest time between sets, you won’t be out of breath as much, etc.
Fat loss
Most likely, you are interested in Cardarine (GW 50156) just because of the fat loss benefit.
Similar to increasing endurance, Cardarine provides us with the benefit of fat loss in two different ways:
- Increased oxidative capacity in muscles – This means that we will burn more calories when exercising than we normally would without Cardarine.
- Suppression of Glucose metabolism – switching energy source from Glucose to fat. – This one is pretty self-explanatory. By switching the energy source from glucose to fat, we are able to directly burn off fat instead of first burning off the excess glucose that our body stored. In fact, the effect is very similar to a very strict ketogenic diet, but without actually doing the diet.
Lot’s of animal testings done on rats proved Cardarine helps a lot when it comes to fat loss. The studies showed that the rats that were on GW 50156 dropped 5% body fat more than the rats that weren’t taking the compound.
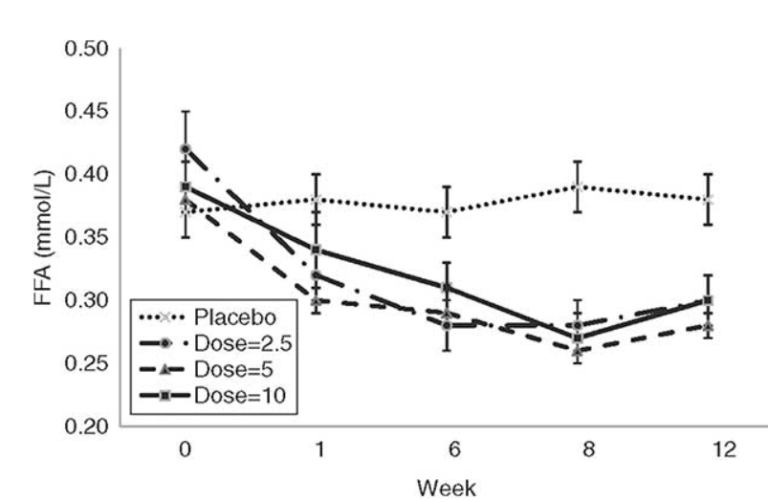
According to a study that tested Cardarine on 13 obese men with high body fat percentage and an unhealthy lipid profile. Just 2.5mg of Cardarine reduced their LDL, triglycerides and fatty acids.
In my experience, most people are able to drop 5-7% of their body fat over the course of an 8-week Cardarine cycle. You will be able to lose fat even when on a calorie maintenance diet or a slight calorie surplus. However, for the best results, I recommend that you stick to a slight calorie deficit diet during your GW 50156 cycle.
Remember, when it comes to fat loss, your diet and training will make the biggest impact. You can take as much of Cardarine as you want, if you have a bad diet, it won’t make much of a difference.
Improved Cardiovascular health
This is actually one of the main reasons Cardarine was researched and developed, to treat cardiovascular diseases.
Studies and animal testings on rats showed that GW 50156 has a very positive effect on our cardiovascular system. It reduced the damage done to rats, improved their blood vessels and reduced inflammation.
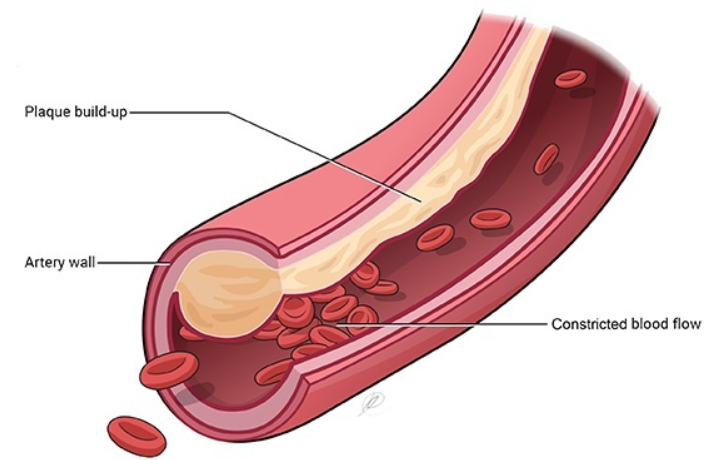
Even low doses of Cardarine were shown to clear up blood vessels which lowers the risk of heart attack and other cardiovascular diseases. GW 50156 was shown to be effective at removing the plaque build-up in blood vessels.
In fact, some steroid users who take very strong steroids that are hard on your cardiovascular system, like Trenbolone, often take Cardarine so that they can avoid damaging their cardiovascular system and can stay healthy.
I will most likely use small dosages of Cardarine when I get older (over 50 years old) because of this benefit. It will allow me to have a very healthy cardiovascular system.
My recommended companies for buying Cardarine
Improved liver and kidney health
Not a lot of people know this, Cardarine has a very positive effect on our liver and kidneys. This is really amazing because most similar compounds are actually liver or kidney toxic.
For kidneys, Cardarine showed that it reduces inflammation and studies found out that it lowers the chances of developing kidney disease.
GW 50156 also reduced the inflammation in the liver. It also switches the energy source from glucose to fat which is shown to improve our insulin resistance and this is beneficial for our liver and is obviously very beneficial to people who are struggling with Diabetes.
Cardarine side effects
Now that we have gone over the benefits of GW 50156, let’s take a look at the side effects.
Cardarine went through a lot of studies and research. So far, only one side effect was revealed and that is:
- Accelerated development of cancerous tumors
The 2007 GSK (GlaxoSmithKline) conducted a study that showed an accelerated cancerours tumor development in rats that were taking Cardarine.
Some people are very skeptical of this study because they used absurd dosages of Cardarine for extremely long cycle periods. Since 2007, there have also been a lot of studies that are contradictory to the one that showed cancer development. Basically, the whole thing is a bit controversial.
Let’s go over this in-depth and explain when you should and when you shouldn’t worry about this.
Cardarine cancer
The thought of Cardarine accelerating the development of cancerous tumors is the reason why a lot of people aren’t using it even though it might be great for them. But are we really in the risk of developing cancer if we cycle GW 50156?
As of 2024, there have been 0 cases of documented cancer in people linked to Cardarine. Still, you need to be carefu and know everything about this compounds correlation to cancer. Let’s dive right in.
When it comes to the topic of Cardarine causing cancer, we have a lot of studies to look at.
On one side, we have the study that most of you already know. It was responsible for the discontinuation of Cardarine in 2007. Basically, it showed that the rats who were given Cardarine experienced fast development of cancerous tumors.
On the other side, we have a bunch of newer studies that proved that Cardarine doesn’t cause cancer at normal dosages for normal cycle length. In fact, the studies proved that at normal dosages, Cardarine has anti-cancer properties.
These studies are:
To better explain this, let’s first go over cycle length and the dosages that the rats were given in the 2007 study.
What Cycle Length And Dosages Did Rats Get
A lot of people and a ton of websites claim that the rats were given a huge amount of Cardarine. Some of them are just listing random numbers like 50x, 70x, or even 100x the recommended dosage. But what dosages did they actually get?
The lowest dosage at which neoplastic was found in rats (neoplastic is just another word for tumors or cancerous tumors) was at 3mg a day.
Now let’s turn this 3mg a day dosage in rats to a human equivalent dosage (HED). We will use the human equivalent dose calculation based on body surface area from ResearchGate (picture below).
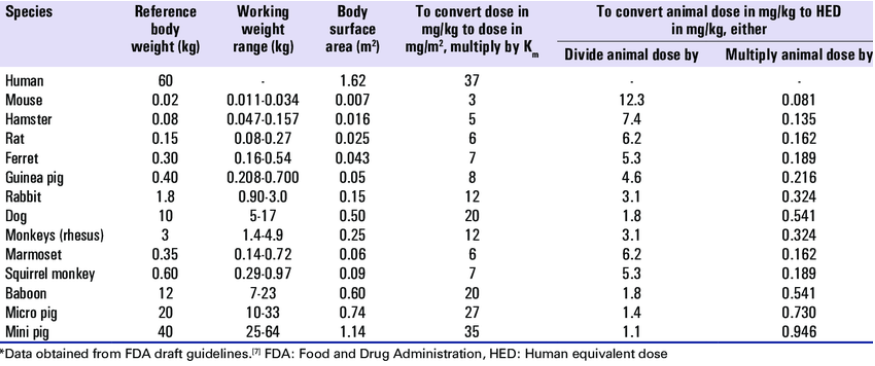
Human Equivalent Dose(mg/kg) = Animal Dose(mg/kg) x [Animal Km / Human Km]
= 3 x (6/37)
= 0.48 mg/kg
Where Animal Km is 6 for rats, and 37 for humans, and 3mg is the lowest dose where neoplastic findings were found.
For a 190 pound / 85 kg person, this is the equivalent of 40.8mg per day. Or 43.2mg per day for a 90kg person.
So as you can see, the dosages used were about 4x bigger than the recommended dosages, not 100x or 50x as some people claim.
Another important thing is the cycle length used in the study. The study ran for 104 weeks, which is about 13x more than the maximum recommended cycle length of 8 weeks.
To summarize, the dosages used in the infamous rat study were 3x higher than recommended and the length of the study was 13x longer than the recommended cycle length.
Keep in mind that it took all of this, 3x higher dosages, and an absurd cycle length for cancer to show up.
If you take normal dosages and stick to normal cycle length, you will almost certainly be fine. Some recent studies even confirm this, let’s look into them.
Cardarine Has Anti-Cancer Properties – Study
This GW 50156 study proved that Cardarine doesn’t cause cancer at high dosages and short cycle lengths.
I recommend that you read the study for yourself if you are interested, it’s very long and in-depth. If you don’t have the time, however, let me summarize it for you.
Neither GW compound increased cell growth or phosphorylation of Akt and no increase in the expression of VEGF or COX2 were detected in any cancer cell line in the presence or absence of serum. Similarly, liver, colon and colon polyps from mice administered these compounds did not exhibit changes in these markers.
Essentially, this study proved that Cardarine doesn’t cause the development of cancerous tumors even at high dosages for normal periods of time. Not only that, the compound was shown to actually have some anti-cancer properties in this period.
They used dosages comparable to taking 154mg a day as a 90kg person. These high dosages didn’t show any signs of cancer development at cycle lengths of 7 days.
Basically, this means that high dosages for normal periods of time won’t cause cancer and we could assume that the reason cancer occurred in the 2007 rat study was because of the absurd cycle length (104 weeks), not the high dosages or maybe a combination of the two.
Cardarine Cancer – Conclusion
Let’s summarize the topic of GW 50156 causing cancer.
Yes, Cardarine can cause cancer, but only if taken at high dosages (over 40 mg a day) for a very long period of time (104 weeks in the case of 40mg a day). Obviously, a 100mg a day dosage could cause cancer sooner, at 50 weeks.
If you take Cardarine correctly and stick to normal cycle lengths and dosages, you wont have any problems. In fact, a study actually proved that GW 50156 actually has anti-cancer properties if taken accordingly.
This redditor also adds a very nice point to all of this:
As of 2024, there have been no documented cases of cancer in humans linked to Cardarine. I assume that this is the case because nobody is taking it for 104 weeks straight at 40mg a day.
Make sure to follow these two rules to be safe:
- Normal cycle length (maximum of 8 weeks)
- Normal dosages (maximum of 15-20mg a day)
Human trials
Contrary to popular belief, there have been many GW 50156 human trials done and no, none of them got cancer.
There were three Cardarine human trials:
These human trials showed that Cardarine isn’t liver toxic as there were no changes in the liver that could demonstrate damage.
Also, there were significant, very positive, changes to HDL, cholesterol, and triglycerides. The second and third studies also saw improvements in insulin sensitivity and a decline in fatty acid ~20%.
Not only that, but these human trials also saw a big improvement in body composition. However, body fat% data wasn’t captured so there is no clear data on that.
An interesting thing about these human trials is that some groups were given dosages of 10mg a day for 12 weeks. These dosages gave all of the mentioned benefits and didn’t show any side effects.
Because of this, a lot of people, including me, take Cardarine at 10-15mg a day for 8-week cycles without worrying.
My experience with Cardarine
I have taken multiple cycles of Cardarine of 15mg a day for 8-weeks. I really like this compound especially because it has literally no side effects if you take it this way, two studies confirmed that it won’t cause anything to do with cancer for periods and dosages like this.
The last time that I took it, I stacked it with a small dosage of 10mg a day of Ostarine. This let me to easily get rid of all my fat and keep all my muscle mass (even gain some). It easily leaned me out, I lost my fat and dropped to about 9% body fat from 15 or 16% body fat. Keep in mind, I was careful with my diet and training as well.
Overall, this is a great compound in my eyes. I absolutely love the endurance benefit, it makes cardio easy for me. Not to mention all of the healing properties of Cardarine for the liver, kidneys and heart. I would say it’s very similar to Stenabolic but I feel like it is more effective at fat loss and endurance gain.
My cycle:
Week: 1-8
Cardarine: 15mg a day, Ostarine: 10mg a day
If you want to read my in-depth review, read my article about Cardarine results.
GW 50156 PCT
As we said, Cardarine isn’t a SARM. It is also non-hormonal and won’t cause us to have a suppressed natural production of Testosterone.
This means that we don’t need a PCT (Post Cycle Therapy) for Cardarine. PCT is actually a very serious thing and can have serious side effects. This is why we shouldn’t do a PCT if we don’t need to. You definitely need a PCT with steroids but with SARMs that’s not the case.
Cardarine before and after results
Now that we’ve covered my experience with this compound, let’s go over some real Cardarine reviews and results from other people.
We will go over the results from two people, if you want to read more reviews from other people, read our article about Cardarine before and after. There we go over more before and after pics and their Cardarine cycles.
Cardarine Results #1

His cycle:
| Week | Cardarine |
| 1-8 | 20mg a day |
This is a good example of what you can expect to see from your Cardarine cycle. He (the person in the photo) lost about 5% body fat and managed to keep most of his muscle mass.
Train at least 3-4 times a day as well as have a moderately clean diet and you will easily be able to achieve results like this using the same cycle as he did.
Cardarine Results #2

His cycle:
| Week | Cardarine | Ostarine |
| 1-8 | 15mg a day | 10mg a day |
As we can see, this is an example of a Cardarine – Ostarine cycle. He achieved decent results, nothing spectacular though. You should easily be able to achieve and surpass results like this with a decent diet and hard training. The person in the photo lost a few % of body fat and probably gained about two lbs of muscle mass.
You should be able to achieve results like this even without the help of Ostarine
Stacking GW 50156 with SARMs
Cardarine is non-hormonal, it won’t cause any suppressed production of natural Testosterone. This means that we can easily stack it with any SARM without problems or complications.
We actually recommend that you stack it with SARMs like Ostarine or LGD-4033, depending on what you are trying to achieve. If you want to put on lean muscle mass and no fat, we recommend LGD-4033 and if you want to cut and keep all your muscle mass you should stack it with Ostarine.
Cutting and Bulking cycles
We will go over two Cardarine cycles. Cutting cycle and bulking cycle. Both of these examples are using SARMs with GW 50156. Keep in mind that if you want, you can cycle only GW 50156 as well.
Cutting cycle:
This is a great cutting cycle, it will let you keep all your muscle and put on some as well. You will easily lose your fat and be full of energy. Don’t forget that diet and training will be very important, we can’t avoid that. We won’t need a PCT for this cycle. Ostarine is really mildly suppressive, our body will easily recover naturally in a few weeks after the cycle.
The cycle:
| Week | Cardarine | Ostarine | PCT |
| 15mg a day | 10-15mg a day | / |
Lean bulk cycle:
This example is a great lean bulking cycle. We will gain only lean muscle and lose some fat at the same time as well. Keep in mind, training and diet will be very important, we won’t be able to avoid that. We also won’t need a PCT for this cycle. The LGD-4033 dosage isn’t high enough to cause problems and our bodies will easily be able to recover naturally after the cycle.
The cycle:
Week: 1-8
Cardarine: 15mg a day, LGD 4033 2.5-10mg a day, PCT: no PCT
Cardarine Dosage
We recommend that you run a dosage of 10-25mg of Cardarine a day to see the best results. Beginners should obviously start at 10mg and work their way up. Dosages like were also shown to have no signs of risk of cancer so this is why we recommend that you stay in this range.
You should cycle Cardarine for 8-weeks. Some people do 12-weeks without problems but we still recommend 8 because a study that we mentioned earlier showed that this cycle length is safe and has no side effects.
For more information about this, check out our Cardarine dosage guide.
Cardarine half life
GW 50156 has a half-life of 24 hours. This means that in order to keep the optimal levels of Cardarine in our body (to get the best possible results), we should take a dosage once every 24 hours. If you forget a dosage, don’t worry, just take the normal dosage (not a double) the next day and continue your cycle normally.
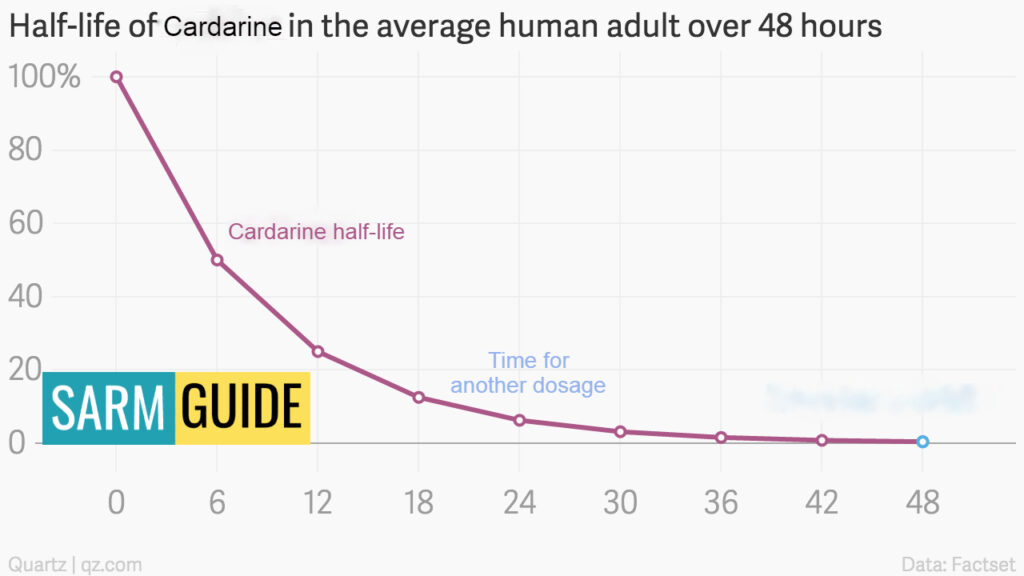
Some recent studies have shown, however, that the half-life of Cardarine might be somewhere between 10-24 hours.
So that is why you can even take it a step further by splitting your dosage into two parts. Studies have shown that this is actually superior to taking one dosage a day. Although the difference is not that big, it’s still worth trying.
Take the first part in the morning and the second part in the evening. So for example, if you are taking 20mg of GW 50156 a day, take the first 10mg in the morning and the second 10mg in the evening.
You can read more about this in our article about Cardarine half-life where we answer the questions like; the best time to take GW 50156, etc.
When does Cardarine kick in
A lot of people aren’t sure how fast Cardarine actually kicks in. It’s important that we know this so that we can easily tell if our Cardarine is bunk or not.
Increased Endurance
When it comes to the increased endurance, Cardarine starts working in about 20 minutes after the first dosage and lasts throughout the whole cycle. Usually, the endurance starts gradually going down after the cycle, but if you do a lot of cardio even after the cycle, you can manage to keep most of the endurance.
Increased endurance is also a very easy way to tell if your GW 50156 is real. If you don’t get an increased endurance after the first dosage, try increasing your dosage. But if you still don’t get an increase in endurance even when you try 25mg a day, for example, you almost certainly have a bunk product.
Cardiovascular Health
The increased cardiovascular health also comes in very fast, in the first two weeks. Obviously, we can’t see this without doing a blood test, but it’s still good to know that our cardiovascular health will improve fast.
Some people who are using compounds that give our cardiovascular system a hard time (trenbolone, for example), love to use Cardarine because it makes it safe. They say that according to their blood tests, GW 50156 makes a huge positive difference in blood pressure, cholesterol levels, etc. in only a week.
Fat Loss
Most people, however, are interested in the fat loss benefit. That takes a little bit longer to kick in compared to the endurance or the increased cardiovascular health. In my personal experience, you can expect to see the first signs of fat loss in the first two to three weeks of the cycle. Obviously, if you train hard and keep an eye on your diet, you will notice it faster.
On average, though, if you eat at calorie maintenance and train decently often, you will see fat loss progress by the end of the second or third week.
Tip: Take frequent photos of yourself, this way you will have an easy time tracking your progress.
Where to buy Cardarine
Obviously, if you want good results and no side effects from a compound like Cardarine, you have to make sure that you have high-quality, pure compounds. Some companies sell products like SARMs and GW 50156 but actually put very little of the actual compound into their products and put something else in there instead, like prohormones. This can obviously have serious side effects and won’t bring you the results you want.
This is why it’s so crucial that you buy your GW 50156 and other compounds from trusted companies that don’t sell bunk products.
I recommend that you buy your Cardarine from my recommended company. I tested their Cardarine and I can guarantee that it is pure and high-quality. You will experience incredible benefits from their compounds and won’t experience any side effects.
Plus, they have a 90-day money-back guarantee if you aren’t satisfied with the products, so you have nothing to lose.
My recommended companies for buying Cardarine
Conclusion
In conclusion, Cardarine is a great product that has incredible benefits like:
- endurance
- fat loss
- improved cardiovascular health
- improved kidney and liver health
A lot of people are scared off because people talk about cancer when they talk about GW 50156. In reality, this compound won’t cause cancer at normal dosages at all. Recent studies have shown that the infamous Cardarine rats most likely got cancer because of the absurd cycle length (2 years).
Also, Cardarine is amazing when we stack it with compounds like Ostarine or LGD-4033. We can cut and keep all our muscles or bulk without putting on any fat. But don’t forget, these compounds aren’t magical pills that will let us do whatever, training and diet will still be very important and the most important factor for our results.
Don’t forget that you should always buy your compounds from trusted sellers like my recommended companies, this way you can be sure of what you are getting.
FAQ About Cardarine – GW 50156
Let’s go over some FAQ (Frequently Asked Questions) about Cardarine ( GW 50156) and answer them.
What Is Cardarine (GW 50156)?
Cardarine is a PPARδ receptor agonist that has benefits like improved endurance, cardiovascular health, fat loss as well as improved kidney and liver health.
How Does Cardarine (GW 50156) Work?
Cardarine will switch our energy source from glucose to fat. This means that we will burn off more fat and we will have more endurance.
What Is The Proper Cardarine Dosage?
The proper Cardarine dosage is between 10-25mg a day. Beginners should start at 10mg a day.
What Is Cardarine Half-Life?
The half-life of Cardarine is 24 hours. This means that we should take one dosage every 24 hours for the best results.
What Side Effects Does Cardarine Have?
A study found that Cardarine can cause the development of cancer. Keep in mind, the study used 50x the recommended dosage for 2 years straight.
Is Cardarine Legal
As of 2024, you can legally buy and use Cardarine in every country in the world except for Australia. In Australia, it’s considered as a Schedule 9 compound by the TGA which means that it’s illegal even with a doctor’s prescription.
Does Cardarine Actually Work
Yes, Cardarine absoluletly works. In fact, it’s so effective that people feel it as soon as 20 minutes after the first dosage.
What is Cardarine used for
Cardarine is mostly used for fat loss because of its fat loss benefits. A lot of professional athletes, however, also use it for the benefit of increased endurance
Cardarine vs GW0742
Some people mistake GW 50156 with GW0742. They are actually the exact same compounds with one difference. GW0742 has one less Hydrogen atom but it has one more Flurione atom.
It was developed by GlaxoSmithKline as a “new version of Cardarine”. As of 2024, GW0742 has no animal or human studies.
A lot of companies are selling Cardarine but very few are selling real, pure GW0742.
Find out more about GW0742 by reading our in-depth GW0742 review.
